


Myth Busting With the SC joint
- Admin
- Aug 31, 2020
- 11 min read

Updated: Sep 1, 2020

When was the last time you considered the sternoclavicular (SC) joint when working with a patient? If someone doesn’t complain of pain or clicking in this area do you check it off your list of things to consider from a movement perspective?
As the articulation between the medial aspect of the clavicle and the manubrium of the sternum, the SC joint is classically described as a synovial, saddle-shaped joint. You’ll find out in this blog post that its structure and function are more complex.
The SC joint helps the clavicle function as a bony strut between the sternum and the scapula, allowing for our great ability to reach away from our body. It’s claim to fame as the sole skeletal articulation between the axial skeleton and the upper limb is more than a fun fact.
When contemplating the kinematics and pathology of the shoulder complex we obsess over scapular movement. The kinematics of the SC joint are described in textbooks but rarely consider clinically.
If the sternoclavicular joint is more involved in movement and function than many of us give it credit for, why is this the case? I believe the reason is multifactorial, due in part to insufficient information but also misconceptions about the joint and broader topics in the realm of movement science.

This post is another opportunity to question our beliefs and do some myth busting, this time with the sternoclavicular joint. (Click here and here for other myth busting)
MYTH # 1

Many believe that less relative motion equals less significance in the bigger picture of movement. That might be true in some contexts but definitely wrong as a blanket statement.
Part of the reason this joint gets ignored lies in the paucity of (recent) research.
In fact, the most frequently cited study on SC joint movement was published almost 60 years ago by Inman et al.(1)

Hitherto, we need more research on this joint
The truth is that the SC joint moves quite a bit (in concert with the AC joint). This coordination is what leads to larger movements of the glenohumeral joint and the scapula and on the thorax.
SC joint osteokinematics are described via the resulting motion of the clavicle.
Elevation/Depression - in the frontal plane
Protraction/Retraction – in a horizontal plane
Posterior Rotation – in a (near sagittal plane)
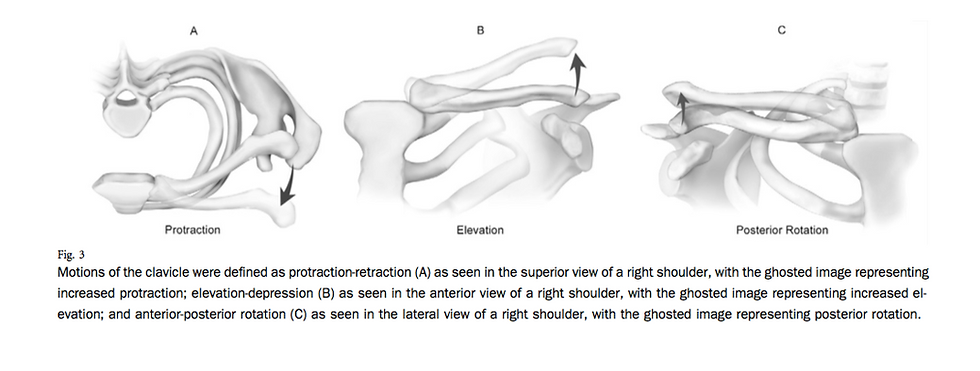
image from Ludewig et al (2)
In their in-vivo study of the 3D kinematics of the SC joint, Ludewig et al demonstrated that during maximum arm elevation the SC joint accounts for
6 degrees of elevation
16 degrees of retraction
31 degrees of posterior rotation (2)
In addition to lack of information there is also conflicting information.
MYTH # 2

Maybe not quite 50 shades, but there is a decent amount of “grey” when it comes to the known arthrokinematics of this joint.
As a movement practitioner, if movement potential is lacking you want to find out how and why. Sometimes it is a “joint” problem. To test joint play one must have an understanding of arthrokinematics. At least that is what we’ve all been taught.
With regards to arthrokinematics of the SC joint most agree on the intricacies of clavicular elevation/depression and posterior rotation.
During elevation of the clavicle the articular surface ROLLS superiorly and SLIDES INFERIORLY on the sternum. The opposite happens with clavicular depression
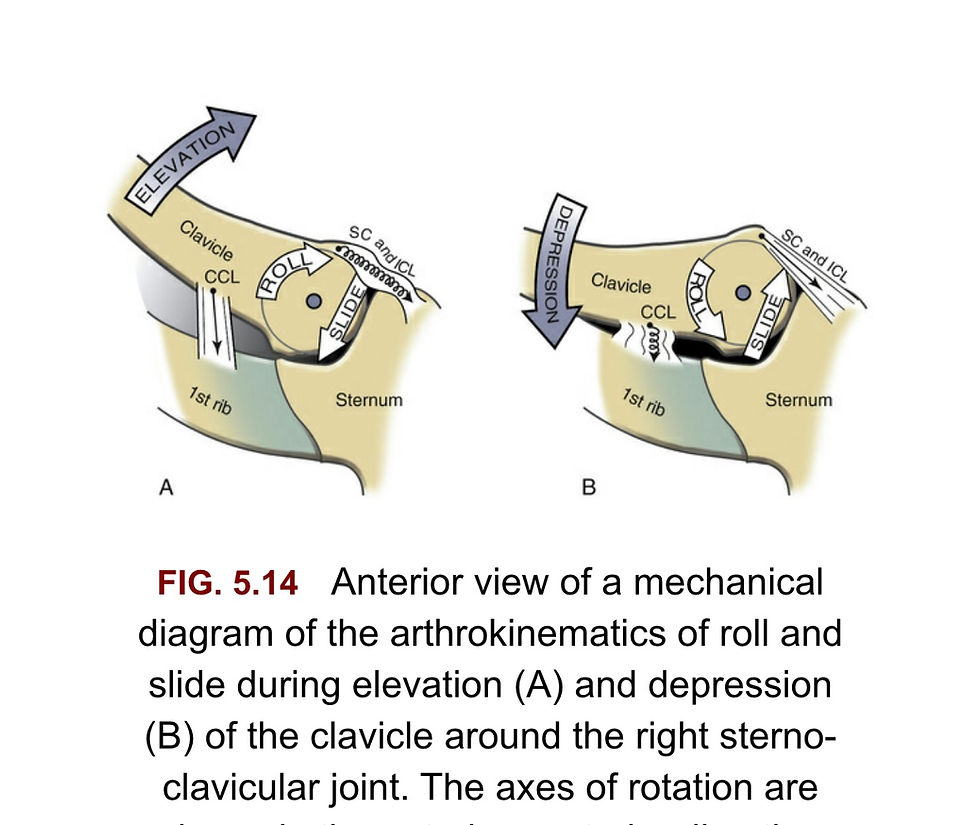
image from Neumann (3)
As the clavicle posteriorly rotates, the clavicle’s sternal end spins relative to the lateral surface of the articular disc.
When it comes to the mechanics of protraction and retraction things are less clear.
Kinesiology expert Don Neumann describes the joint mechanics of protraction and retraction as such (3):
Protraction: The clavicle both rolls and slides ANTERIORLY
Retraction: The clavicle both rolls and slides POSTERIORLY
When researching for this post, I discovered there are conflicting views on the arthrokinematics of the SC joint for protraction/retraction. I’d say sources were mixed, 50-50. I actually learned the opposite of Neumann’s description. (i.e., for protraction the clavicle will roll anterior but glide posteriorly)
Inconsistency can be confusing so I sought clarification by emailing shoulder expert Paula Ludewig, PT, PhD. The majority of kinematic research on SC joint, AC joint and scapula over the last 10 years bears her name.
Here is her response to my question:

Until we have more research data what do we do with uncertainty? Not evaluate joint play because there might not be a “NORMAL”?
These questions lead us to another grey zone – the rules (or principles) we are taught for manual therapy.
MYTH #3

If there is arthrokinematic variability how do we assess this joint? And if we even consider manual therapy as an intervention, what rules apply?
I think the answer might lie in the debate over the concave-convex rule. Did you know it was even up for debate?
As a main tenant taught in manual therapy, the concave-convex rule can be more accurately described as a principle. In reality, it is more of a theory based on observations of how structure and function correlate. The concave-convex rule is intended to assist a practitioner in determining the direction of mobilizing glide.
The problem is multiple kinematic studies show the arthrokinematics described in the rule don’t always apply. Examples include radial head movement during supination at the proximal radial-ulnar joint (4), femoral translation during deep knee flexion (5) and humeral head translation during external rotation (6) (with adhesive capsulitis) and abduction.(7)

Sometimes Myths (Like Rules) Are Made For Breaking
Neumann tackles this topic in a 2012 editorial in the Journal of Orthopedic and Sports Physical Therapy.(8) He argues that the intention of the concave-convex rule is to provide a description of how a joint might roll and slide to optimize joint centration rather than a directive for manual therapy. With this in mind, one would still assess joint play (as part of a more comprehensive exam) and mobilize in the direction of restriction.
Neumann also brings up an important point when reflecting on the contradicting studies. Starting position matters, or simply stated, position matters.
MYTH #4
Our (understandable) love affair with movement has lead to a neglect of static measures of position.
Movement is the behavior we consistently assess in the hope that we can manipulate its variables to enhance resiliency. There is more to the story. Static measures of position help us understand how the axial skeleton has self-organized with years of adaptations. They can explain why motion is limited at a joint and why other systems are responding in a particular way.
For the SC joint we can use the following to accrue information:
The clavicular resting position (relative to the horizontal plane)
The angle the clavicle makes with the plane of the scapula
We must remember two important things when we consider these metrics.
There is likely variability based on the influence of a number of factors.
These measures are made relative to something else, meaning they are influenced by and potentially affect something else.

The clavicular resting position:
Chaitow cites 25-30 degrees as “normal” (9)
Ludewig et al found the mean to be 19 degrees (+/- 5 degrees)- (2)
When considering movement at the SC joint we can use this position measure as a starting point for clavicular movement.
The clavicular resting position may be influenced by or affect the resting scapular position:

image from Kapandji (10)
The angle the clavicle makes with plane of the scapula, observed from a cranial to caudad perspective is another measure of relative position that can give us information about the SC joint.

image from Kapandji (10)
Several sources cite 60 degrees as normal and in terms of SC joint movement, should be considered when contemplating how the scapula and clavicle move together.
The picture below (of a melon and kitchen tongs) demonstrates how the shape of a thorax, narrow or wide A-P) might influence this angle both at rest and with movement.

Other factors that may influence this angle include adaptations to trauma at the clavicle or surrounding structures. To understand movement you need to appreciate structure and position but it's also crucial to know a person’s history.
MYTH #5

“What’s the value of a subjective history when you are a movement specialist?”
I’ve heard this asked several times. Beyond identifying yellow and red flags, I believe the subjective component to an assessment is the key to understanding findings and connecting dots.
With respect to the SC joint, medical history might include incidents of trauma.
Clavicular fractures account for up to 45% of fractures in the shoulder complex and 2.6% of fractures overall. They often result in malunion and are frequently treated conservatively. (11)
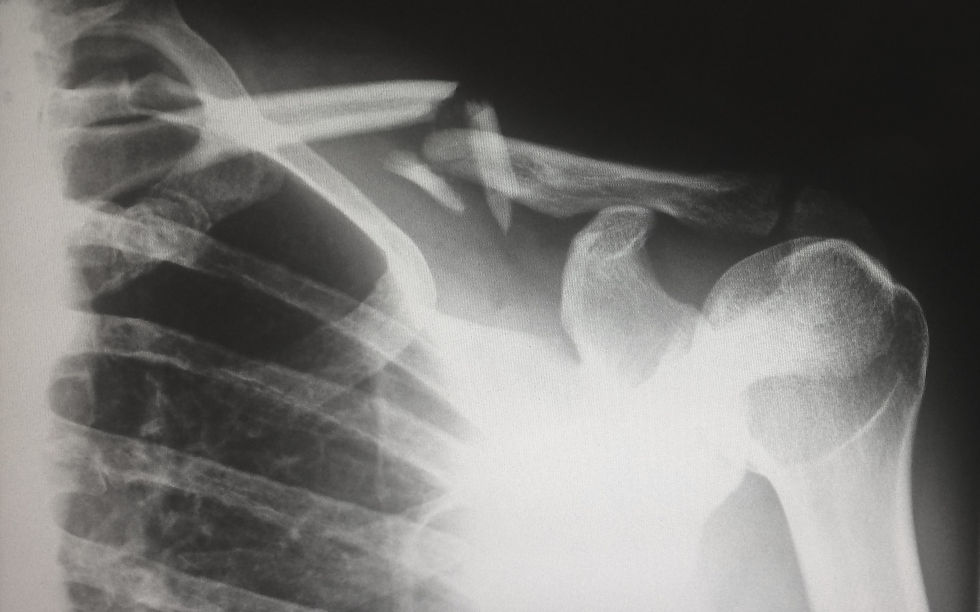
Two potential consequences of a malunion include clavicular shortening and/or axial displacement.
Shortening of the clavicle by up to 20mm has been reported. The subsequent changes to the relationship between the clavicle and its connections with a change like this could alter the kinematics of the entire shoulder complex. In fact, malunions that result in clavicular shortening by 15 mm have been shown to orient the scapula more anteriorly on the thorax.(12)
Interestingly, the clavicle develops at a slower rate than most long bones in the body. It is the first long bone to begin ossification but the last to complete it. One must consider the potential for bone growth disruption with any trauma history especially prior to 20 years of age.

While clavicular fractures are relatively common, traumatic injuries to the SC joint are rare. Graded as a sprain, subluxation or dislocation these injuries typically occur as the result of a fall or motor vehicle accident.
Anterior dislocations are far more common than posterior dislocations, thankfully. There is a lot more than joint integrity that can be affected by a posterior dislocation including the vagus and phrenic nerves, trachea, esophagus and multiple important blood vessels.

As a synovial joint, non-traumatic pathologies also occur at the SC joint. These include relatively common presentations of osteoarthritis, rheumatoid arthritis and psoriatic arthritis. For a good review of pathologies affecting the SC joint check out this article (13) and this Clinical Edge podcast with physiotherapist Jo Gibson.
If you see a SC joint that appears swollen, warm and painful with no history of trauma, refer to a medical doctor. Considering the region of pain or discomfort you will also want to consider the following in your differential diagnosis – acid reflux, hernia, and the various other diagnoses that can result in chest pain.
The issue with trauma to the SC joint and/or clavicle is not always that the joint becomes “unstable” but that it changes the relative position of the clavicle at rest and consequently it’s starting point for movement.
MYTH #6

Cited as an integral part of the shoulder complex, the SC joint is rarely recorded as a component of the thorax.
Not only does the articulating component of the manubrio-sternum warrant this, so does the connection the clavicle has with the first rib. Several sources describe this articulation as the sterno-costo-clavicular joint, the SCC joint. In addition to the connection via the costoclavicular ligament an actual synovial joint has been shown to exist in up to 20% of individuals. (14)
Using what we know about anatomy, physiology and kinesiology one can critically reason that the sternoclavicular joint impacts more than shoulder movement. Looking at the connections the medial clavicle has to the upper airway and the thorax it makes sense that the SC joint might affect function in these areas as well.
Breathing
While no specific studies have investigated how the SC joint moves with respiration, we can combine what we know about anatomy and the kinematics of breathing to develop some hypotheses about what may happen.
Contributing factors such as the crank shape of the clavicle and it’s articulation with the manubrium and the first rib one can speculate that as the manubrio-sternum moves some movement occurs at the SC joint.
The articulation of the clavicle with the sternum exists in close proximity to the clavicle’s articulation with the first rib (right next to and on the first costal cartilage). When the manubrium moves during respiration it pulls the first rib with it as a unit. Studies show that during inhalation the sternum moves in anterior and superior direction. (15)
Assuming “normal” position and mechanics in the thorax and shoulder complex, pump handle mechanics of the sternum and upper ribs likely lead to a reciprocal posterior rotation of the clavicles.
Leon Chaitow inverts the relationship, describing sternal movement in physiologically normal breathing as being “allowed for” by the SC joint. Looking at things from multiple angles is important. (9)

Out of the box thinking is sometimes hard to swallow
Swallowing
Dysphagia is a symptom that might also be related to SC joint pathology. Although rare, there are examples in the literature that cite mechanical obstruction linked to the sternoclavicular joint as a causative factor.
Two case studies describe such a linkage. One proposed dysphagia caused by the mechanical influence of a posterior osteophyte secondary to SCJ osteoarthritis. (16) A second paper cited dysphagia in 2 cases of septic arthritis affecting the SC joint. (17) In these cases the authors speculate that the inflammation present caused compression on the subjects’ esophagus.
What neither case study mentions is that lying in this same region, and potentially relevant to the dysfunctional swallowing, are the infrahyoid muscles. Both the sternohyoid and sternothyroid attach to the proximal end of the clavicle, near (and in the case of the sternohyoid muscle ON) the SC joint.

image from Kapandji (10)
It is possible that osteophytes and/or inflammation in these cases may have impacted muscle function of the infrahyoids, which serve to stabilize the hyoid during swallowing.
And not to get a head of myself but the hyoid bone is intimately connected to the cranium so keep that in mind.
CONCLUSION
My interest in writing this post started out as a biased view that the SC joint was not appreciated or often assessed. After hours of research it’s clear to me that we need a better understanding of the SC joint. We need to push for research on its role in movement and it’s potential role in regions beyond the shoulder complex.
Movement is complex. We observe and measure limitations in isolation but we must consider them in the dynamic contexts with appreciation of one’s adaptive history. These adaptations in turn may affect multiple systems of our body.
My goal is to have you check your biases and consider the SC joint more than you did yesterday. Probabilities of an issue at the SC joint is dependent on someone’s history but learning and appreciating these connections may help solve difficult cases.

I don’t mean check your own SC joint- Check your biases
References
1. Inman VT, Saunders JB, Abbott LC. Observations on the function of the shoulder joint. J Bone Joint Surg Am. 1944;26:1-30.
2. Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, LaPrade RF. Motion of the shoulder complex during multiplanar humeral elevation. J Bone Joint Surg Am. 2009;91(2):378-389.
3. Neumann DA, Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 3rd ed. St. Louis, MO: Mosby/Elsevier; 2016.
4. Baeyens JP, Van Glabbeek F, Goossens M, Gielen J, Van Roy P, Clarys JP. In vivo 3D arthrokinematics of the proximal and distal radioulnar joints during active pronation and supination. Clin Biomech (Bristol, Avon). 2006;21 Suppl 1:S9-S12.
5. Scarvell JM, Hribar N, Galvin CR, et al. Analysis of Kneeling by Medical Imaging Shows the Femur Moves Back to the Posterior Rim of the Tibial Plateau, Prompting Review of the Concave-Convex Rule. Phys Ther. 2019;99(3):311-318. doi:10.1093/ptj/pzy144
6. Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis. J Orthop Sports Phys Ther. 2007;37(3):88-99. doi:10.2519/jospt.2007.2307
7. Baeyens J-P, Van Roy P, Clarys JP. Intra-articular kinematics of the normal glenohumeral joint in the late preparatory phase of throwing: Kaltenborn's rule revisited. Ergonomics. 2000;43(10):1726-1737. doi:10.1080/001401300750004131
8. Neumann DA. The convex-concave rules of arthrokinematics: flawed or perhaps just misinterpreted? J Orthop Sports Phys Ther. 2012;42(2):53-55.
9. Chaitow L, Bradley D, Gilbert C, Recognizing and Treating Breathing Disorders. 2nd Ed. Churchill Livingstone. 2013
10. Kapandji AI, The Physiology of the Joints: The Upper Limb. 7th Ed.Scotland. Handspring Publishing 2019.
11. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002;11(5):452-456.
12. Michael Ledger, Nicole Leeks, Tim Ackland, Allan Wang, Short malunions of the clavicle: An anatomic and functional study, Journal of Shoulder and Elbow Surgery,Volume 14, Issue 4,2005, Pages 349-354.
13. Edwin J, Ahmed S, Verma S, Tytherleigh-Strong G, Karuppaiah K, Sinha J. Swellings of the sternoclavicular joint: review of traumatic and non-traumatic pathologies. EFORT Open Rev. 2018;3(8):471-484. Published 2018 Aug 25. doi:10.1302/2058-5241.3.170078
14. Paraskevas GK, Koutsouflianiotis KN, Iliou K, Syrmos N, Ioannidis O, Noussios G. Costoclavicular Joint: An Osteological Study on Clavicles with Clinical Relevance. Cureus. 2019;11(4):
15. Beyer B, Feipel V, Sholukha V, Chèze L, Van Sint Jan S. In-vivo analysis of sternal angle, sternal and sternocostal kinematics in supine humans during breathing. J Biomech. 2017;64:32-40.
16. Gill JR, Morrissey DI, Van Rensburg L, Tytherleigh-Strong G. Sternoclavicular joint osteophytosis: a difficult diagnosis to swallow. BMJ Case Rep. 2017;2017:bcr-2016-219053
17. Das AK, Monga P. Septic arthritis of the sterno-clavicular joint as a cause of dysphagia: a report of two cases and review of literature. Clin Rheumatol. 2014;33(1):141-143
Photo credits:
Shane, Harlie Raethel, Umberto from Unsplash



Comentários